Did MIS-C Ever Really Exist?
How a clinical syndrome with no specific test became a generation-defining pediatric emergency, and then quietly vanished

I am reminded infrequently now, but still often enough, about the fog of war that prevailed during the COVID pandemic. Everyone now says we made mistakes and should acknowledge those mistakes so we never make them again, but the same people struggle to clarify what those mistakes were. There is just this handwaving about “being better”. Be specific, I want to scream, tell me exactly what the passage of time has confirmed we got wrong. Medicine is, of course, complicated and the lay public should now understand that certainty in biology is hardly like the certainty of physics, but that does not mean we cannot know things. So let us spend some time together on the curious disease entity known as MIS-C that arrived to prey on children during the pandemic, and as quickly as it arrived, was gone.
The story is told like this: SARS-CoV-2 was generally mild in kids, but a small subset developed a terrifying delayed hyperinflammatory syndrome called multisystem inflammatory syndrome in children, or MIS-C. This syndrome killed dozens of American children, hospitalized thousands more, and provided one of the most important reasons to vaccinate every child in the country. Then, thanks to vaccines, MIS-C all but disappeared.
This is, at best, half true. At worst, it is a textbook case of a syndrome that was conjured into existence by clinician attention, sustained by definitional looseness, and then dissolved back into the pre-existing diagnostic categories from which it was drawn.
The single most important fact about MIS-C, the one that should appear in the first paragraph of every news article ever written about it, is this: there is no test for MIS-C. No biomarker, no imaging finding, no genetic signature, no autoantibody, no histologic feature. The diagnosis is entirely clinical, made by exclusion, in a setting where the exposure criterion — evidence of prior SARS-CoV-2 infection — became universal in the pediatric population by 2022.
When a disease has no specific test, the question of whether the disease “exists” in any given patient is really a question of whether the clinician decided to apply the label. Surveillance counts of such a disease are not counts of a biological phenomenon. They are counts of decisions. So its worth carefully exploring what the basis for that clinical decision was.
The case definition
Here is what CDC required, in its May 14, 2020 Health Alert Network advisory (HAN-00432), for a child to be reported as an MIS-C case:
Age under 21.
Fever >38.0°C lasting ≥24 hours, or report of subjective fever lasting ≥24 hours.
Laboratory evidence of inflammation — including but not limited to elevated CRP, ESR, fibrinogen, procalcitonin, D-dimer, ferritin, LDH, IL-6, neutrophilia, lymphopenia, or low albumin.
Clinically severe illness requiring hospitalization, with multisystem (≥2) organ involvement: cardiac, renal, respiratory, hematologic, gastrointestinal, dermatologic, or neurologic.
No alternative plausible diagnoses.
Positive for current or recent SARS-CoV-2 infection by RT-PCR, serology, or antigen test; or COVID-19 exposure within the four weeks prior to symptom onset.
Notice that nothing in the diagnostic list picks out a disease. Every individual criterion is extremely non-specific. Fever? Inflammatory markers that go up in almost any serious illness in a child? Multi-organ involvement describes any sufficiently sick hospitalized patient. The SARS-CoV-2 criterion, by 2022, was met by essentially every child in America — pediatric seroprevalence crossed 75% by mid-2022 and approached universality thereafter. That leaves criterion 5: no alternative plausible diagnosis. This is not a criterion for a disease, rather a criterion for a clinician’s verdict. MIS-C, by this definition, operationally meant “a sick febrile child with inflammation and a positive COVID antibody whose doctor decided not to call it something else.”
Embedded in the same advisory, two instructions that are relevant to the case I‘m going to make:
“Some individuals may fulfill full or partial criteria for Kawasaki disease but should be reported if they meet the case definition for MIS-C.”
“Consider MIS-C in any pediatric death with evidence of SARS-CoV-2 infection.”
The first instruction tells clinicians to relabel Kawasaki disease as MIS-C whenever the “COVID criterion is met.” The second tells them to consider MIS-C in any pediatric death with a positive SARS-CoV-2 test or antibody — which, by 2022, meant essentially every pediatric death in America, because every child had antibodies. The diagnostic substitution was not an emergent methodological accident. It was a written instruction from the agency. The death count is being padded by bureaucratic nudge.
The CDC eventually acknowledged this was a problem. In January 2023, the case definition was revised — tightened, in their language — to require an elevated CRP specifically (≥3.0 mg/dL) rather than the prior menu of inflammatory markers, and to drop renal, respiratory, and neurologic involvement from the qualifying organ system list. The agency's stated reason for dropping respiratory involvement was that "respiratory organ system involvement is more common in COVID-19 than in MIS-C and its inclusion in the MIS-C case definition may contribute to misclassification." Translation: for three years the surveillance system had been counting severe acute COVID as MIS-C, and CDC quietly fixed it. The 2023 definition also added an explicit instruction that "if documented by the clinical treatment team, a final diagnosis of Kawasaki Disease should be considered an alternative diagnosis. These cases should not be reported to national MIS-C surveillance" — meaning the entire formal boundary between MIS-C and Kawasaki disease, in CDC's own surveillance language, reduces to which label the treating clinician chose to write down.
The agency's own validation work, published in MMWR in December 2022, retroactively applied the new 2023 case definition to MIS-C cases reported through August 2022 and found that 13.0% of cases counted under the 2020 definition did not meet the 2023 definition. The same analysis showed that a substantial fraction of 2020-era cases had qualified only through respiratory, neurologic, or renal organ involvement — exactly the criteria CDC was dropping in 2023 because, in the agency's own words, those features overlapped too heavily with acute COVID. Thirteen percent of accumulated surveillance data, retroactively, did not represent what CDC now thought MIS-C was.
The hits keep coming. A 2024 paper in Pediatrics by Day-Lewis and colleagues at the esteemed Boston Children’s Hospital — senior authors include Jane Newburger, one of the country’s leading Kawasaki disease researchers, and Mary Beth Son of the *Overcoming COVID-19* network — performed an analysis at a single institution. Of 119 children diagnosed with MIS-C using the 2020 definition, 20 (17%) did not fulfill the 2023 definition. Six of those 20 (30%) had shock or cardiac involvement — these were not trivial cases. In the same study, of 59 patients given a clinical diagnosis of Kawasaki disease at the same institution during the same period, 10 (17%) simultaneously met the 2020 MIS-C definition. The two diseases, by the CDC’s own criteria during the surveillance period that generated the famous numbers, overlapped on roughly one in six patients.
The same paper provides the data point that calls into question the antibody criterion that had been proposed to be used as a meaningful discriminator of KD and MIS-C. Of the 112 Boston Children’s patients with serologic testing — kids clinically diagnosed with either MIS-C or Kawasaki disease during the pandemic — 109, or 97%, were SARS-CoV-2 antibody positive. Including the kids clinically labeled as classic Kawasaki disease. In a population where 97% of children presenting with KD-like illness at a major academic pediatric center had positive COVID antibodies, the antibody criterion does not help whatsoever in distinguishing MIS-C from Kawasaki. It is met by essentially every patient in the differential.
This is not just a methodological critique. The data points it rests on come from Boston Children's, published in the AAP's flagship journal, by authors who include the country's leading Kawasaki researcher and a senior investigator in the Overcoming COVID-19 network. None of those data points have been challenged in the year since.
What the phenotype of decedents tells us.
The sword of Damocles that public health hung over parents’ heads was that a beautiful, healthy child could be suddenly struck down by this rare but fatal post-viral syndrome. The data refute the framing. The children who died of MIS-C were overwhelmingly not healthy children. They were the medically fragile children who have always died in pediatric ICUs. Bowen and colleagues at CDC, in the first peer-reviewed analysis of MIS-C decedents (35 deaths among 2,818 cases through March 2021), found that 69% of decedents had one or more underlying medical conditions versus 38% of survivors. Preexisting neurologic disease was associated with 5.1-fold increased odds of death (95% CI 1.9–14.1); noncardiac congenital abnormalities with 6.5-fold increased odds (95% CI 2.6–16.0). Obesity was present in 46% of decedents. Among decedents, 71% had pneumonia, 46% had acute respiratory distress syndrome, and 86% required vasopressors for shock. The lethal phenotype was severe pneumonia and septic shock physiology in children whose underlying medical conditions had long made them vulnerable to exactly this kind of acute infectious mortality.
The implication is that the MIS-C case definition was lumping together two populations. One — the mucocutaneous-phenotype survivors — clinically resembled Kawasaki disease, responded to Kawasaki treatment, and had low mortality. This population is biologically real; whether it constitutes a discrete syndrome distinct from Kawasaki spectrum vasculitis triggered by SARS-CoV-2 remains contested in the pediatric rheumatology literature, but it is not the population public health was warning parents about. The other population — the respiratory-failure decedents — was dying of severe pneumonia and septic shock physiology, in medically fragile children, often with severe pre-existing conditions. Whether what killed them was a post-viral hyperinflammatory sybdrom from SARS-CoV-2 or an unrelated acute infection that the surveillance system reflexively labeled MIS-C because the antibody criterion was universal — is a question CDC never answered.
CDC itself acknowledges the limitation that breaks the entire mortality attribution: in the Bowen 2021 paper, the authors concede that "information about specific causes of death was not collected." The national surveillance system tabulating MIS-C deaths never documented what the children actually died of. The deaths were attributed to MIS-C because the patients had met MIS-C clinical criteria during their final hospitalization, not because anyone adjudicated MIS-C as the proximate cause of death.
What the lethal MIS-C phenotype actually was
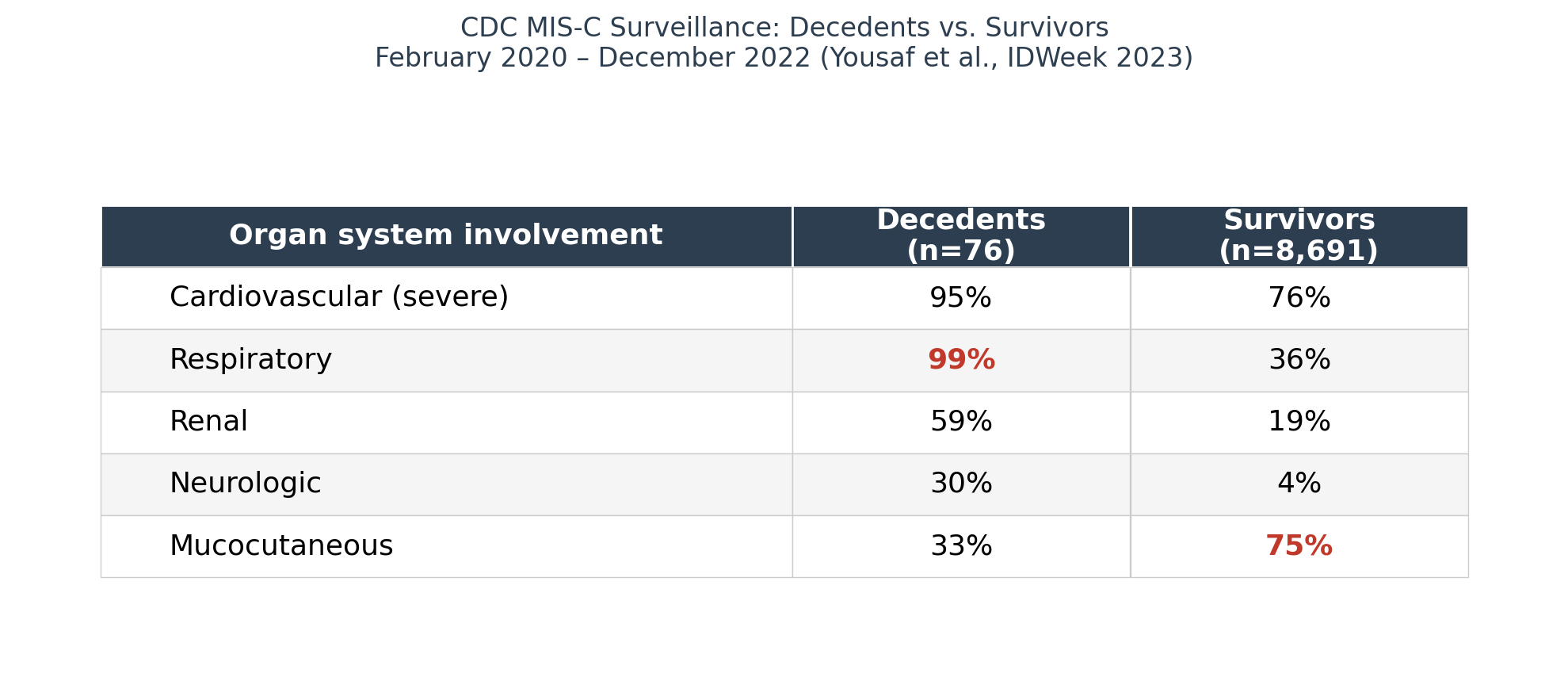
Putting the pieces together. The CDC decedent population:
99% had respiratory involvement, often dominant
95% had severe cardiovascular involvement (consistent with septic shock physiology)
59% had renal involvement (consistent with shock-induced acute kidney injury)
Only 33% had mucocutaneous features
51% had underlying medical conditions (well above the survivor rate)
This is not the clinical picture of post-infectious hyperinflammatory MIS-C. This is the clinical picture of severe acute community-acquired infection causing sepsis and respiratory failure in medically vulnerable children. The infection in question is almost certainly not SARS-CoV-2, because these children had peak post-COVID immunity at the moment of their presentation. It is something else — most plausibly the usual roster of pediatric respiratory pathogens that have always killed medically fragile kids.
The pandemic-era contribution to this population’s mortality was the relabeling, not the dying. These kids would have died in 2018 or 2024 just as surely as they died in 2021. The MIS-C label is what got attached to them in the surveillance system because the criteria allowed it and the institutional attention demanded it.
Diagnostic substitution at the lethal end
Unlike what the CDC and public health establishment did by anchoring to only one possibility — MIS-C — let’s go through all the possible causes of the 79 cumulative deaths through April 2024. They were almost certainly a mixture of three distinct populations:
Group A: Kawasaki-spectrum vasculitis triggered by SARS-CoV-2, with rare deaths. These are the mucocutaneous-rich cases that died despite IVIG and other treatment. Kawasaki disease has always killed children at low rates, especially in cases with severe coronary involvement or treatment failure. The pandemic’s contribution is concentrating these cases in time, not creating them.
Group B: Severe acute non-COVID infections in vulnerable children, mislabeled as MIS-C. These are the respiratory-failure decedents with high comorbidity rates — RSV, influenza, bacterial pneumonia, sepsis from various sources. The COVID antibody made them MIS-C-eligible; the multi-organ failure of sepsis filled in the criteria. Pre-pandemic, these kids died of “acute respiratory failure, etiology unclear” or “sepsis, source unclear” without generating a national news story.
Group C: Genuine post-infectious shock from SARS-CoV-2 specifically — the discrete entity the public was warned about. This is what would actually be a new pediatric COVID harm if it existed as a separable category.
The CDC has never disaggregated the 79 deaths along these lines, because doing so would require acknowledging that the case definition was overinclusive at the lethal end and that the public health communication implicitly conflated three distinct phenomena. It would also require acknowledging that “pediatric COVID killed kids from MIS-C” is, for the majority of those deaths, a misattribution.
The biomarker desert
If MIS-C were a real, discrete disease entity, you would expect five years of intense international research to have identified something specific to it. Hundreds of millions of NIH and EU research dollars have flowed into this question. The yield, after half a decade:
T-cell receptor Vβ21.3 expansion was promoted as an MIS-C-specific immune signature in early papers. It was subsequently found in severe Kawasaki disease and toxic shock syndrome. Not specific.
Anti-SARS-CoV-2 spike antibody titers are higher in MIS-C than in mild COVID, but heavily confounded by recent infection and vaccination status. Useless diagnostically.
Autoantibody panels — anti-endothelial, anti-cardiolipin, various nuclear antigens — heterogeneous between patients and overlap with Kawasaki, MAS, and systemic JIA.
Cytokine profiles — IL-6, IL-10, IL-17, IFN-γ all elevated. Also elevated in Kawasaki. Also elevated in sepsis.
Proteomic and transcriptomic signatures have been published in Nature and elsewhere. None has been translated into a validated clinical assay. The discriminator performance is generally against healthy controls or mild COVID — not against the actual differential diagnosis.
In summary — There is no FDA-cleared diagnostic test for MIS-C. There is no validated biomarker panel. There is no specific imaging finding. There is no histopathologic feature. A 2024 pediatric hospitalist evaluating a sick febrile child has exactly the same diagnostic toolkit available as the 1985 hospitalist, plus a SARS-CoV-2 antibody test that returns positive on almost every child and therefore conveys no information.
The closest anyone has come to a diagnostic tool is the KIDMATCH algorithm, published in Lancet Digital Health in October 2022 by Lam, Burns, Newburger, and colleagues across UCSD, Boston Children’s, Rady Children’s, and several other major pediatric centers. KIDMATCH is a deep-learning model that distinguishes MIS-C from Kawasaki disease using patient age, the five classic clinical KD signs, and 17 laboratory measurements, with a reported AUC of 0.91 on internal validation.
Consider what that means. The authors themselves, writing in a peer-reviewed paper, state plainly that “Early detection of MIS-C is a challenge given its clinical similarities to Kawasaki disease and other acute febrile childhood illnesses.” This is the world’s leading Kawasaki research group, collaborating with the country’s premier pediatric cardiology programs, acknowledging in print that clinicians at the bedside cannot reliably distinguish MIS-C from Kawasaki disease or from other febrile pediatric illnesses without algorithmic assistance. They built the algorithm precisely because human clinical judgment was inadequate to tell these diseases apart.
The MIS-C surveillance cases that generated the famous 9,684 number were diagnosed by pediatric hospitalists across the country who did not have KIDMATCH — and who were not blinded to vaccination status when making the call. Whatever diagnostic accuracy they achieved was worse than what the algorithm achieves, in a setting where the clinician’s pre-test probability for MIS-C was shaped by everything the CDC had told them about who was supposed to get this disease. The case count was generated by a process that the field’s own leadership documents as unreliable enough to require AI to fix.
The numbers, and what they actually represent
CDC's final tally, as of April 29, 2024: 9,684 MIS-C cases, 79 deaths.
The 9,684 cases are a count of label applications, not pathological events. This is a smorgasbord that includes:
Cases that would have been called Kawasaki disease in any year before or after the pandemic
Cases of severe acute COVID-19 that were reclassified as MIS-C because the lab work fit the menu
Cases of severe non-COVID infection in children who happened to have positive COVID serology (universal by 2022)
Cases of toxic shock and severe bacterial illness that got the MIS-C label because the workup didn’t return a clean alternative
Cases that actually represent whatever distinct hyperinflammatory phenomenon may exist downstream of SARS-CoV-2
The last group is the only one that corresponds to “MIS-C” as a real biological entity. Its size is unknown. It is certainly smaller than 9,684, possibly much smaller.
The 79 deaths are subject to the same problem. The lethal phenotype is dominated by severe respiratory failure in medically fragile children. The most likely explanation is that the majority of the 79 deaths were from acute non-COVID infections in vulnerable children, mislabeled as MIS-C because the COVID antibody was becoming universal and the surveillance criteria were broad.
This brings us to the most consequential downstream use of the MIS-C numbers: the claim that COVID vaccination prevented MIS-C cases and deaths, and that this prevention justified universal pediatric vaccination.
Problems with the vaccine claim
Return to the lethal MIS-C phenotype, which we've established is largely composed of severe acute non-COVID infections in vulnerable children who happen to have COVID antibodies. If that's right, then:
The mechanism by which vaccines would prevent these deaths is unclear, because the deaths are not caused by SARS-CoV-2. A flu vaccine would do more to prevent flu pneumonia in fragile children than a COVID vaccine would.
The “deaths from MIS-C prevented by COVID vaccination” estimates that have been cited in pediatric vaccine policy are partly counting deaths that were not related to COVID in the first place.
The remaining deaths — Group A (Kawasaki-spectrum) and Group C (true post-COVID shock) — are the population in which COVID vaccination could plausibly do anything.
There is a deeper methodological problem the agency has never addressed. In any observational study comparing rates of an outcome between vaccinated and unvaccinated groups, the outcome has to be measured accurately for the effect estimate to mean anything. When the outcome is a clinical label rather than a biological measurement, and when the clinician applying the label knows the patient’s vaccination status, you get what epidemiologists call differential outcome misclassification — the error rate in measuring the outcome differs systematically between exposure groups. This bias can manufacture effects that have no biological reality.
To play it out concretely: A vaccinated child presents to the ED with fever, rash, conjunctivitis, elevated CRP, and a positive COVID antibody. The attending pediatrician, who has been taught by the CDC for years that MIS-C is concentrated in the unvaccinated, thinks “Kawasaki disease” or “viral syndrome” and works the patient up accordingly. The same patient, unvaccinated, walks into the same ED with the same presentation, and the attending thinks “classic MIS-C.” The patient is identical. The biological event is identical. The label is different. The surveillance system then dutifully reports that MIS-C is concentrated in the unvaccinated, and this gets used to justify continued vaccination.
There is no test that can adjudicate this and no biomarker that can reliably shift the clinician’s pre-test probability. The vaccine efficacy estimate is structurally guaranteed to show an apparent benefit regardless of whether vaccines do anything biologically, because the labeling rule itself moves cases out of the vaccinated bucket and into the unvaccinated one. The CDC has never published a validation study that would let us estimate the size of this bias, because no such study is possible without a gold-standard test, and there is no gold-standard test for MIS-C.
The honest version of the claim that has actually been demonstrated by the surveillance data is this: children diagnosed with MIS-C are more often unvaccinated, in a system where unvaccinated status increases clinician probability of applying the MIS-C label, and where the disease has no specific test that could adjudicate the question independently of clinician judgment. That is not vaccine efficacy. It is a circular argument with the labeling rule doing all the work.
The counterfactual that already happened
The cleanest test of whether COVID vaccination was actually responsible for the disappearance of MIS-C is to ask what happened to MIS-C rates after pediatric COVID vaccine uptake collapsed. CDC and AAP continued to recommend annual COVID boosters for all children through 2024. Pediatric uptake of those boosters was effectively zero — under 10% of American children received the updated 2023-2024 vaccine, and uptake in children under 5 — the age group at highest historical risk for MIS-C in the Omicron era — was around 2-3%.
If COVID vaccination were a meaningful causal factor in MIS-C reduction, this near-total collapse in pediatric vaccine uptake should have produced a continual resurgence of MIS-C. And yet MIS-C cases continued to decline through 2023 and 2024 in a population that was overwhelmingly unvaccinated against COVID and getting more so every month. The CDC quietly stopped tracking the syndrome in May 2024.
Imagine the alternative scenario: the recommended pediatric booster had achieved 70-80% uptake — the kind of coverage childhood vaccines normally achieve in this country — and MIS-C had vanished on the same timeline it actually vanished. The public health establishment would have declared total victory. The MMWRs would have been triumphant.
The press releases would have written themselves: “Pediatric COVID vaccination eliminates MIS-C in the United States.” The booster would have been written into the routine childhood immunization schedule on the strength of that single ecological correlation, cited for the next twenty years as one of the great public health successes of the pandemic response.
That headline was averted only because parents stopped vaccinating their children for COVID. The natural experiment that ran was the one the establishment did not want to run, and the result was that MIS-C disappeared anyway. The variant evolved. The pediatric population developed infection-induced immunity. The syndrome the experts had said required vaccination to control vanished, even in the unvaccinated population.
The establishment now faces a problem it has not addressed publicly: the intervention they recommended turned out to be unnecessary for the outcome they were claiming to prevent. They cannot run the headline that vaccination eliminated MIS-C, because vaccination did not happen and MIS-C was eliminated anyway. So they say nothing. The MIS-C tracker comes down quietly. The annual pediatric booster recommendation continues, decoupled from any of the original justifications for it.
What this means
MIS-C may turn out, in the historical accounting, to have been one of the cleanest examples of a clinical syndrome that was substantially constructed rather than discovered. There was almost certainly something real underneath it — a subset of children, exposed to a novel virus that their immune systems had never seen, mounted delayed Kawasaki-spectrum vasculitis responses that, in rare cases, were severe. That subset existed. It was probably small. I suspect given the methodological issues I’ve chronicled, it represents a fraction of 9,684.
The bulk of the official MIS-C count, and particularly the bulk of the deaths, was almost certainly a relabeling exercise. Pre-existing pediatric inflammatory and infectious mortality, occurring in a population where every child now had a positive SARS-CoV-2 antibody, got channeled into a new surveillance category that had no specific diagnostic criteria and no biomarker to constrain it. The institutional incentives — to demonstrate a discrete pediatric COVID harm, to motivate pediatric vaccination, to justify federal surveillance funding — pushed cases into the bucket. The label gave the appearance of a coherent epidemic. The label disappeared because the institutional attention disappeared, not principally because the underlying biology changed.
The 79 deaths are real children who died, and this is not meant to minimize the tragedy every death represents. But the question of how many of those children died from a discrete syndrome that would not have existed in nosological terms before the pandemic — versus how many died from pre-existing pediatric mortality patterns that the surveillance system relabeled — is an important question that is genuinely unanswerable from the way the CDC comported itself. The agency owes the public better than 9,684/79 with no asterisk, no decedent disaggregation, no specificity analysis, and no acknowledgment that the case definition was overinclusive at the end of the severity spectrum where the deaths were concentrated.
The deeper lesson is about how syndromes can get manufactured during periods of crisis. A nonspecific clinical definition, applied during a period of intense surveillance, in a setting where the diagnostic exposure criterion eventually becomes universal, generates a count that makes an outbreak look much worse than it actually is. There are players who benefit when a crisis looks worse than it is. The interventions the public health establishment was prepared to demand required public fear, and the MIS-C surveillance system was structured to deliver that fear in pediatric form.
Everyone agrees the COVID response was a disaster. But we need to be more specific about what went wrong. Doing so requires clarifying the historical record. Otherwise, prepare for the same playbook to be run again.
Anish Koka is a cardiologist writing on Medicine and Health Policy. He is on X @anish_koka, and hosts a weekly podcast : The Doctor’s Lounge.
I have to quibble with this passage. "The single most important fact about MIS-C, the one that should appear in the first paragraph of every news article ever written about it, is this: there is no test for MIS-C. No biomarker, no imaging finding, no genetic signature, no autoantibody, no histologic feature."
I currently suffer from a post-viral syndrome colloquially known as Chronic Fatigue Syndrome which also has no biomarkers and no tests, its diagnosis is also somewhat of a process of exclusion. I was a healthy and fit young man when I contracted this syndrome, I now need a power wheechair to check my mailbox. I have seen 5 doctors and a psychologist, and none of them has any medical solutions for me.
You may very well be correct that MIS-C does not exist, but perhaps you can also acknowledge that medical knowledge is not perfect, and that there are syndromes which people suffer from which we have absolutely no test nor cure for, even despite many years of research.
Excellent post- thank you. This story is a case study of how diagnostic uncertainty can be used to benefit those with vested interests. With no specific biomarkers, an inflammatory syndrome can be called just about anything. This is why the sepsis gurus have been floundering for so long. I am not a Pediatrician but have wondered about the quoted frequency of severe COVID illness in kids. Without the foundation of having solid diagnostic agreement, we sure as hell should not have been embarking on draconian public health measures based on very dubious declarations of disease activity in America’s youth.