
It is ever more clear that there are two realities emerging about COVID. One echo chamber can be found in the New York Times, that regularly runs stories quoting credentialed modeling experts with doctorates and masters degrees that became popular because they knew exactly what society needed to do to crush COVID the last 2+ years. The other group consists of weary citizens and physicians who have been wading elbow to elbow in the real world for the last two and a half years that view any continued measures to attempt to ‘crush’ COVID as meaningless and probably harmful. The schism can be typified by a New York Times article that ran earlier this week decrying the continued, ongoing tragedy of COVID… and a virtual townhall in Los Angeles given by physicians who actually take care of patients in hospitals.

The New York Times thinks the United States is on its way to a minimum of 100,000 ppl dying yearly from COVID. Meanwhile, the internal townhall on the State of COVID at a major hospital in Los Angeles notes they have no one severely ill with COVID. Presumably, the vast majority of ppl are sick or dying with COVID, not because of COVID.
The remarkable thing is, this has been relatively obviously happening to most of the country for some time now. There is no better leading indicator than US nursing homes which house the sickest, most vulnerable patients in the equivalent of dormitories. The mortality in this group in my native Philadelphia in the Spring of 2020 was the equivalent of a small bomb going off. It was catastrophic.
The COVID waves never ended, of course, but the how the nursing homes fared with those subsequent waves is an interesting story.
In the Fall of 2020 Public health leaders recommended another “slowdown” in Philadelphia in response to rising cases. New restrictions and warnings were planned, and the public schools that had been partially open were to be shuttered in an all virtual mode for the time being.
This was an unfortunate surprise to many who hoped society had learned to live with the virus in some type of a tense Korean peninsula style standoff. Rising case positivity was the buzzword used to describe a pandemic that once again threatened to spin out of control and overwhelm hospitals. But this particular surge had a different flavor than the spring.
As noted earlier, the Spring had been a particularly brutal time for residents of nursing homes. In some states like Pennsylvania, most of the deaths due to COVID were in Nursing Homes.

Figure 1. Nursing Home Deaths in Pennsylvania
Prompted by the Spring devastation in nursing homes, the State introduced a host of rules designed to make nursing homes safer. Many of the mandates mirrored what medical teams had been asking for in March : Universal testing of residents and staff and the ability to cohort COVID positive patients being chief among them.
But something strange happened after mass testing got underway. There were lots and lots of positive results. Unlike March when symptomatic patients that were COVID positive rapidly decompensated and ended up in critical care units, the large majority of the patients that tested positive now seemed perfectly fine. While the Spring saw scores of patients that died, this wave was marked by much less morbidity despite the much larger number of positive patients.
Explaining this fall paradox has much to do with how we track the spread of pandemics in 2020. For the first time in human history disease tracking is happening using PCR, a truly wonderful technology that is, unfortunately not without its limitations. There is simply no escaping trade-offs.
The major problem is that it is simply too sensitive. Any doctor can tell you that the same disease process affects patients in a variety of different ways that are usually beyond the scope of what humans can explain. Coronary disease, cancer, and infectious diseases are indolent affairs in some and raging inferno’s in others. Traditional tracking of pandemic spreads was by tracking how hospitals and mortuaries filled. The yearly influenza waves in the United States gave rise to the U.S. Outpatient Influenza-like Illness Surveillance Network (ILINet) -- a network comprising of ~3000 health care providers that report to the CDC on outpatients seen with a flu like illness, and hospitalization surveillance of laboratory confirmed influenza admissions (FluSurv-NET).
COVID19, however, has been primarily tracked by PCR, and as evidenced by the nursing home protocol implemented in late May, this is happening in completely asymptomatic individuals. Understanding why requires a little review of PCR. PCR works by using small strands of genetic material (primers) designed to be complementary, and highly specific to the target of interest.

Figure 2. PCR Visually explained
False positive PCR tests can result from primers designed for COVID19 not being 100% specific to SARS-COV2, primers annealing to themselves and getting amplified, or sample contamination. Unfortunately, it is not easy to ascertain exactly what the false positive rate is because testing in the United States is incredibly widespread and performed by a variety of labs using different primers and different processes.
But while some very smart experts in PCR have some reliable concerns about the current process, there are a fair number of real world datasets in low prevalence areas that suggest a low false positive rate. The Office for National Statistics (ONS) in the United Kingdom reported 159 out of 208,730 samples were positive between July and September. Even if every single positive test was a false positive that would still suggest a false positive rate of 0.08%. Since the virus is known to be circulating the actual false positive rate is likely to be significantly lower than this. The Aussies down under provide another laboratory because they have largely managed to reduce infection rates to near zero. They also do a fair number of tests. Since mid-May they have been doing 20,000 - 60,000 tests per day in a country of 25 million people.

Figure 3. Low prevalence of false positive tests in Australia as demonstrated by a high background rate of testing (upper panel) and low positive rate (lower panel)
This is true in America as well. Despite the continuous massive testing in a background of very little coronavirus there are remarkably few positive cases. Add to this bevy of data a recent report from Wuhan on the testing of 10 million residents over 15 days that found only 300 asymptomatic cases and it seems fairly likely that there is a high likelihood a positive PCR translates to the presence of Sars-CoV2.
What the Wuhan paper doesn’t do, however, is provide any comfort to those looking for meaning in positive PCRs. All 300 residents that tested positive were asymptomatic and there were no positive tests among 1174 close contacts that were traced. This suggests a certain percentage of positive PCRs are asymptomatic, and don’t transmit virus to others. In essence, these are false positives because they neither bother the carrier of these viral particles or threaten anyone who comes into contact with these carriers.
The achilles heel for PCR is that it doesn't differentiate between live and dead virus, it simply is a fantastic way of picking up minute amounts of viral RNA. Interestingly, the number of PCR cycles required for the test to be positive may provide some clues to the live-dead problem.
Jaafar and colleagues published a research letter in Clinical Infectious Diseases, that sought to correlate Cycle threshold (Ct) values with the ability to grow the virus in culture from a sample of almost 180,000 patients tested for Sars-Cov2. At Ct of 25, up to 70% of patients are positive in culture, and at Ct of 30 this drops to 20%. At Ct of 35 , a value commonly and widely used to report a positive result, less than 3% of inoculated samples grew in culture.
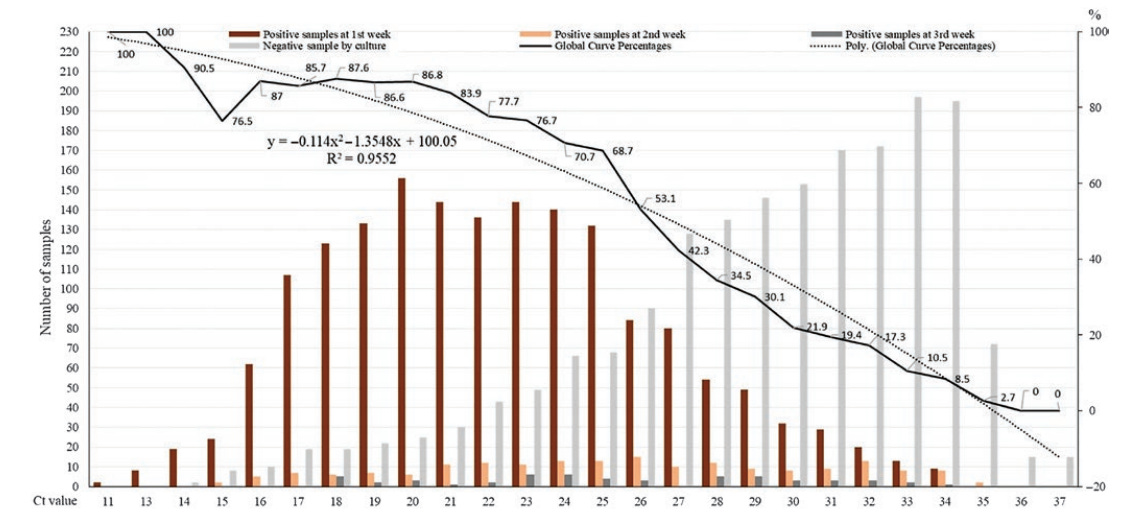
Figure 4. Cycle Threshold (Ct) values correlate with the ability to grow virus in culture. At Ct values > 34, almost no PCR positive samples grow in culture, suggesting PCR positivity beyond this value doesn’t indicate live virus
The problem of course is that this represents one validation study in one lab. At some point there were 2 million tests per day being performed in the United States in a variety of different labs and on a variety of different platforms. The FDA Emergency Use Authorization (EUA) which these tests operate under do provide information on the Ct and Limits of Detection (LoD), but provide no guidance on whether labs should be calling a positive result beyond the Ct at which the LoD was noted.
Curious about positive PCR tests I was seeing in asymptomatic patients, I called the local private lab that was managing the testing for a long term care facility, to inquire about the Ct of these patients. It turns out they were sending their specimens to Labcorp. A few days later I was on the phone with one of the Medical Director’s of Labcorp who was sympathetic, but unhelpful. They were doing hundreds of thousands of tests per day..they didn’t have the manpower to track down a handful of patients for every doctor that called. And no, he also couldn’t produce a general breakdown of Ct numbers for their positive tests.
So in this strange world we live in where testing companies LabCorp and Thermo Fisher did a combined $3 Billion in revenue for COVID testing alone in one quarter, it is impossible in realtime to sort out what percentage of positive tests represent patients with an active infection who can transmit the virus to others. The stakes are not small. Many localities took steps to shut down local businesses and public schools after reaching a certain arbitrary threshold of positive cases.
To be clear, the problem isn’t that cases defined by PCR are meaningless, and have no value, it's that PCR based case spikes may not always mean death and destruction follows. Recall, that the point of massive testing to curb pandemics was to head off spikes in hospitalizations and death. But if a significant portion of the positive cases are of the non-infectious variety, mitigation strategies that are harsh by nature may have pain without the gain.
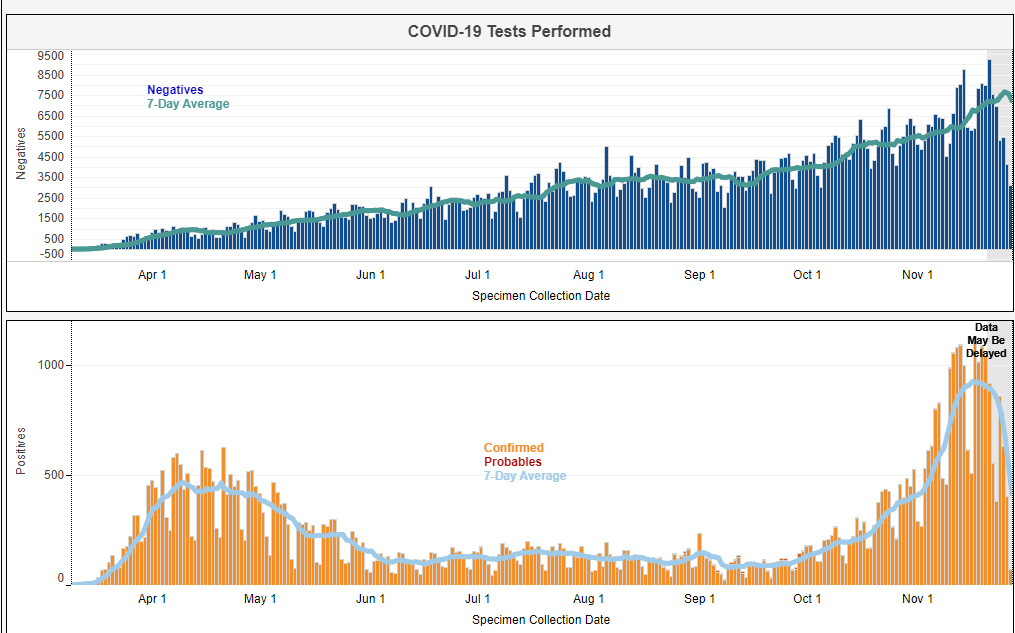
Figure 5. Philadelphia COVID Testing trends March 2020 - November 2020. The expert prediction was that a rapid spike in Fall COVID positive cases would lead to hospitalizations/deaths. This was the rationale used for additional lockdown measures.
The public health expert who isn’t walking the halls of the nursing homes doesn’t know any of this. His ignorance of the relevant local knowledge blinds him to the truth just as the economist Friederich Hayek predicts in his seminal essay describing the necessary ineptness of any central planner faced with complex systems.
The epidemiologist, the bureaucrat and the virologist COVID expert on twitter would come to the natural conclusion that since an avalanche of deaths followed the spike in cases in the Spring of 2020, cases rising even more steeply in the late Fall of 2020 would portend more death that would require societal mitigation measures. It’s only someone that was in the nursing homes observing what was actually happening in nursing homes that would observe the difference in acuity of positive cases between the two surges and consider a different outcome.
Hospitalizations in the Spring of 2020, were not the same as hospitalizations in the Fall of 2020
There were other matters of concern in the fall - hospitalizations were rapidly rising as well. But this, yet again, serves as an important reminder that data aggregators fall far short of those actually involved in the clinical care of patients on hospital wards. When hospitalization rose rapidly in the Spring, elective surgeries were canceled and entire floors were converted to become COVID critical care units because the need for beds was immense. The daily toll of deaths in the Spring in Philadelphia, while never close to New York City’s gruesome die-off of up to 1,000 deaths per day was still ugly.
But what wouldn’t be immediately obvious to the data scientist is that hospitalizations in the Spring of 2020 in Philadelphia were much different than hospitalizations in the Fall of 2020. Doctors were more seasoned, less panicked, and had therapeutics available to them in the Fall they did not have in the early months of the pandemic. Less panicked doctors meant fewer patients placed on mechanical ventilators early in the course of their disease when it was recognized that artificial ventilation was likely increasing mortality. This also translated into much less of a need for precious intensive care beds.
Fall hospitalizations were also marked by patients being admitted for intravenous therapy early in the course of their illness, which again translated into a lower acuity patient population. Elective surgeries that had been suspended during the first wave were restarted as that wave receded. They were never suspended again in any hospital in Philadelphia. In stark contrast, the city of Philadelphia that had married opening businesses to rising cases, and case positivity rates announced a series of restrictions in response to the rising Fall cases. The restrictions include no indoor dining at restaurants, capacity limits at retail stores and religious institutions, telework for office workers required unless it is not possible, a ban on indoor gatherings of any size, outdoor gatherings limited to 10 percent occupancy with a cap of 2,000 people, and no youth or school sports. Colleges, universities, and high schools were also only allowed to offer online classes. In effect, the Philadelphia central planners stopped the world again because they didn’t know positive cases in the fall were different from positive cases in the Spring, or that hospitalizations in the fall were nothing like hospitalizations in the Spring. The feared second wave that was going to make the first spring wave pale in comparison never quite materialized. There was an uptick in deaths, but it was nothing like the first wave.(Figure 6) The astute clinician, and the hospitals with plenty of skin in the game were right. The City planners were wrong.
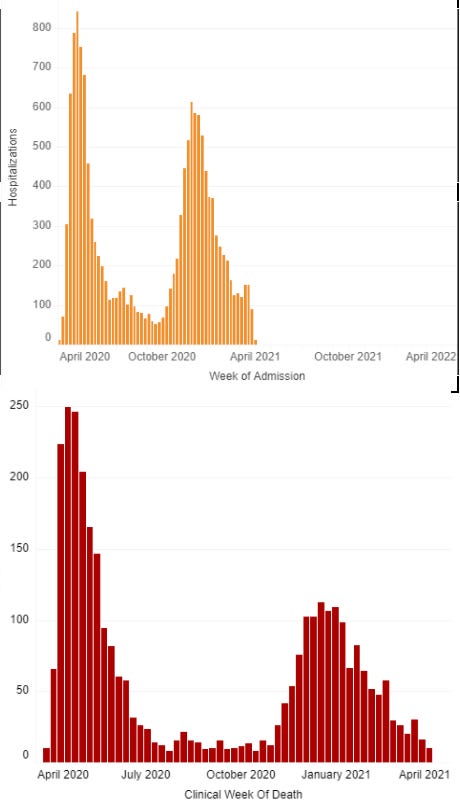
Figure 6. Philadelphia hospitalizations in the Fall did not have the same mortality as the Spring, because patients admitted in the Fall of 2020 were not as sick. Important, because hospitalizations were suggested as a metric for lockdown measures
Keep in mind that these charts of COVID deaths are a bit challenging to parse because every COVID wave will result in more COVID positive patients in the hospital, and some of these patients will die in the hospital with COVID. What has become blindingly obvious to anyone in hospitals is that each recurring wave of COVID has had fewer and fewer patients sick because of COVID, so the COVID hospital numbers have become less meaningful with time. Tying any policy changes to this data has been a shaky endeavor for long before the current video of physicians in Los Angeles making fun of the media’s obsession with COVID was made.
The complex ever changing epistemological landscape of all things COVID underscores the difficulty of translating the acquisition of knowledge into decisions — a topic that has been the subject of debate long before this pandemic afflicted the world. The scale of errors made through action or inaction by those given powers they should never have been given have been dumbfounding. Time and time again it has been those experiencing the pandemic at street level that have taken the body blows dealt by the virus and adjusted accordingly. It was an ophthalmologist in Wuhan that sounded the alarm about the unusual pattern of cases, and it was bureaucrats that attempted to stifle spread of this news. It was the head of the sequencing lab in China that uploaded a sequence of the new viral genome to a public server instead of waiting endlessly for permission from some higher up. The NBA decided to cancel its season before the CDC thought it was a good idea, and it was citizens that rushed to buy n95 when Anthony Fauci was recommended against one. This isn’t unexpected. There are no professionals who manage pandemics of this scale because they happen once every hundred years. The experts anointed to manage this aren’t gifted athletes who have honed their skills by shooting ten thousand free throws, they are mostly titled suits whose job is to confirm the biases of a large enough audience to be called back over and over again. In this world, it is the plugged in art dealer who is right more often than wrong on all things COVID because the ‘expert’ scientists are busy using science as a political tool to play up the existential threat of a brain/lung/heart eating virus that can only be conquered by prophylactic restrictions on basic rights designed with uber eats ordering zoomocrats in mind. It's no accident that the policy designers happen to be zoomocrats.
The stories of COVID exposes the widening gap that social theorist Thomas Sowell wrote about a half century ago between those with first hand knowledge and decision makers. Sowell warned that clueless intellectuals making decisions would not only threaten our economic and political efficiency, but ultimately threaten our very freedoms because a knowledge based society would be replaced with an elitist, abstract, utopic vision of what society should be like.
The lessons from the COVID pandemic should extend well beyond the spread of infectious viruses. There is no intrinsic truth in reams and reams of data being produced by the second. You need people with real knowledge of what’s happening on the ground to interpret the data. As the last 2 years have demonstrated, the alternative path of following the prescriptions of the credentialed, overly confident policy making cult that has been logging in to the pandemic from their bedrooms leads to mayhem and chaos. Lets try not to do that again.
Anish Koka is a Cardiologist. Follow him @anish_koka
Excellent and thoughtful review. Data interpretation and reality divide. Policy makers pay attention!
Thanks for this excellent commentary. As I understand PCR testing, any positive found only at, say, 25-30 cycles amounts to a false positive. To judge from the figures from New York reported in the link below, what we have been through has been, in significant part, an epidemic of misleading test results.
https://www.nytimes.com/2020/08/29/health/coronavirus-testing.html