

The latest CDC paper on vaccine myocarditis is NOT reassuring


Today’s post on the latest COVID vaccine myocarditis paper gets a big assist from the wicked smart data visualization expert Josh Stevenson (subscribe to his substack!)
In August 2021, the CDC began a study to follow-up cases of myocarditis in the age group at highest risk for myocarditis after mRNA COVID-19 vaccination. The survey based study is deserving of a deeper dive, but the date of the publication of these studies is particularly galling because it means the CDC had this data when the Advisory Committee on Immunization Practices (ACIP) — a committee that develops recommendations for the routine administration of vaccines - met a few weeks prior on September 1st to finalize recommendations for the new bivalent mRNA vaccine now available from Moderna and Pfizer.
Certainly, NOT presenting longer term follow-up data on vaccine myocarditis in detail is one way of trying to make sure the ACIP would come up with a clean recommendation on vaccines.
Not surprisingly, the committee ultimately did vote 13 to 1 to recommend the bivalent COVID-19 vaccine made by Moderna for people 18 years of age and older, and the Pfizer bivalent COVID-19 vaccine for those 12 years and older. CDC Director Rochelle P. Walensky, MD, MPH, endorsed the ACIP’s recommendations later that evening. The new boosters are to be given at least two months after receiving the last vaccination.
Frustratingly, there is no robust safety data about the new bivalent booster that contains 50-μg bivalent vaccine mRNA-1273.214 (25 μg each of ancestral Wuhan-Hu-1 and omicron B.1.1.529 [BA.1] spike messenger RNAs). It is possible that this particular booster has a lower, equivalent, or higher rate of myocarditis compared to its predecessor. We just don’t know, and the plan, apparently is to find out by attempting to roll it out to every American > 12 years of age.
So, at the very least a study by the CDC that attempted to follow up a high-risk demographic who were diagnosed with myocarditis after the original mRNA vaccine was administerd should be particularly important to parents and young adults weighing the risks and benefits of taking a mRNA COVID19 vaccine now. The overarching message of the keep-it-simple ethos of public health as it came to the cases of myocarditis that have been reported primarily in young men since April 2021 was to quickly pivot from denying any link existed to referring to myocarditis after vaccines as ‘mild’ and a brief inconvenience.
The current study should dispel the ludicrous notion that clinical myocarditis - a disease entity that comes to light when you have chest pain because cells in your heart are dying — is mild.
The CDC study published in Lancet on previously healthy 12-29 years old’s is a survey-based study. The major limitation of a study based on surveys is that many people (like me) seldom respond to requests for surveys. The final sample ends up being biased in ways that we can’t understand. Knowing the demographic data for those who do not respond may give some insights into how biased the final sample that is included in the analysis is, but is still pretty imperfect.
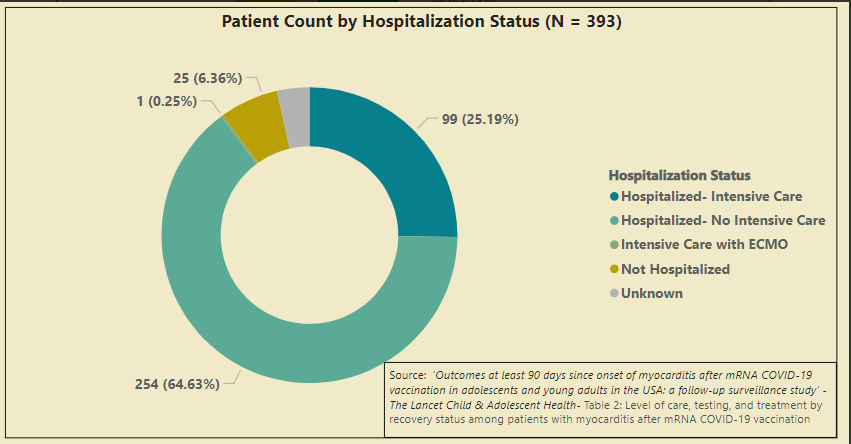
So, of the 989 cases of myocarditis that were identified via VAERS, there is information on hospitalization status for 519 of them. We know that 484 (93%) of them were hospitalized. 393 of the patients had information about the level of care that was needed in hospitals, so from this, we glean that 99 (25%) of the group that was hospitalized needed to go to an intensive care unit. One of these patients ended up requiring massive support using something called ECMO (extracorporeal membrane oxygenation). This is an intervention used only in the sickest of the sick critically ill patients who need a separate machine to take over the normal duties of the heart and lung. It is essentially a modified version of a heart-lung bypass machine that is used commonly when surgeons need to perform heart surgery.
No deaths occurred during the follow-up, but we have no information available for the patients who were eligible but did not respond to the survey. We can charitably assume that no deaths occurred in the survey non-responders, but it isn’t clear to me why anyone should be charitable when there is just no data on 53% of the patients that were eligible for the survey.
As far as the longer-term follow-up, the news is not comforting for a group of presumably formerly healthy children and young adults. Again, we only know about follow-up for 385 of the 836 patients who were eligible to be surveyed by a health care provider regarding a myocarditis diagnosis. Of these 385 patients, 261 patients were deemed fully recovered, 61 patients were improved but not fully recovered, and 59 were deemed probably fully recovered.
This means one-third of patients who had vaccine myocarditis were not fully recovered three months after their diagnosis. “Recovery” is by its very nature subjective, and it is possible that the survey responders are more likely to be patients who have anxiousness or depression. This indeed was the most common health-related quality of life complaint noted: 46% of the responders reported anxiousness or depression.

These subjective symptoms would be less concerning if there was better news related to more objective markers of a return to a prior to myocarditis baseline. Unfortunately, the objective data tracks these symptoms. 122 patients (31%) had some restriction of physical activity at the last follow-up (median ~90 days), and 104 patients (26%) were still on medications.

The final bit of bad news relates to the common laboratory and imaging tests cardiologists typically use to assess for heart dysfunction. The highlights are as follows:
6% still had an abnormal echocardiogram (ultrasound of the heart)
10% still had abnormal troponins (blood test indicative of cardiac cell damage)
53% had an abnormal cardiac MRI
47% had evidence of scarring by cardiac MRI
The abnormalities I’ve chosen to highlight are important because the associated clinical context (a recent episode of clinical myocarditis) makes it very likely the abnormalities found are indeed related to myocarditis, and not random incidentaloma’s being picked up by a too-aggressive screening regimen.
This is an important point misunderstood by many in the medical community. Cardiac MRIs are highly sensitive tests that light up when overused to screen random members of the population. But this group with scars noted by Cardiac MRI based on something called Late Gadolinium Enhancement (LGE) is not a random selection of individuals, these are patients with reasons to have a scar in their heart because they are presenting months after pieces of their heart died due to myocarditis. No one in their right mind (until COVID) would ever think to dismiss scars on a cardiac MRI after a clinical case of myocarditis. These are very likely to be real scars. The valid, open question is what these scars mean long term. And the best answer is that we don’t know.
We know from a nice CDC paper that the amount of cardiac damage with vaccine myocarditis is less than classic viral myocarditis and that acute Sars-COV2 myocarditis in this age group to date has been exceedingly rare, so hopefully, this means the prognosis for vaccine myocarditis is a good one. But a good long-term prognosis related to these cardiac scars is what everyone hopes for, not what anyone knows.
In summary, we have a CDC follow-up study that shows 25% of survey responders with vaccine myocarditis were admitted to the ICU, and one of these cases required a modified type of heart/lung bypass machine to stay alive. The ~90 day follow-up data shows one-third of survey respondents were not fully recovered, a third still had activity restrictions in place, and a quarter of patients were still taking medications. Additionally, the cardiac imaging data suggests almost half of respondents who had cardiac MRIs had evidence of a persistent scar. These were all formerly healthy children and young adults.
I have zero interest in my 18-year-old healthy son that spends his weekends scaling 25-foot walls as part of a college ROTC program, testing the theory that vaccine myocarditis is mild and “probably” has no long-term effects. Given the known risks outlined here with the mRNA vaccines, young men like my son deserve a choice when it comes to taking the next iteration of this vaccine.
This latest data dump did not arrive soon enough to affect the ACIP committee’s recommendations but should serve to chill the ambition of exuberant, overconfident bureaucrats still seeking to mandate vaccines in the fall of 2022.
The words “safe” and “effective” need to be applied only when the work needed to use these words has been done. That work is far from complete.
Anish Koka is a cardiologist. Josh Stevenson is a data visualization expert. Sadly, no bank accounts were padded as a result of this post.
PS. I have to make the obligatory post-script here that I oversaw the administration of hundreds of mrna vaccines starting in March of 2021 in my cardiology clinic. The vaccine efficacy data for the original data was from thousands of patients and I certainly felt given the devastation wreaked on many of my patients in 2020 that the vaccines were the best chance of avoiding morbidity and mortality. The process to get the vaccines from the city department of health was a somewhat arduous 3-month process, and once the vaccines were on hand, there were daily reporting requirements that I dutifully performed for the many months we were administering vaccines. To accommodate the rush of patients, employees, volunteers, and conscripted children worked multiple weekends to administer the vaccines. So, I’m especially disgusted by medical colleagues and others who label any concerns registered about vaccine adverse events as “anti-vaxx”. Registering concern over a vaccine adverse event does not make doctors or patients “anti-vaxx”.
 | A guest post by
|
Megyn Kelly interviewed a couple who lost their son from “sudden death” 4-5 months after his shot. I know it’s not possible to say the vaccine caused this, but it is very tragic that someone even recommended the shot to him. He had antibodies prior to getting it. He was immune. What can we do to stop this insanity? Thank God my teenagers are unvaxed and immune. I regret recommending this unsafe injection for anyone. If that makes me an antivaxxer, so be it. https://podcasts.apple.com/us/podcast/the-megyn-kelly-show/id1532976305?i=1000579973809
I don't understand why people get all hot and bothered with and over people attempting to attach labels to them.
This is my response:
1. Define your accusation/claim
2. Prove it!
If, invariably, they cannot do neither, especially #2, I demand that they pay me $10m they owed me! Then they shut up knowing what would come after that.
Here was an actual example:
Some people got all excited over Fullermich's gabfest. I asked his ardent supporters on Sub for one concrete achievement of his Committee. One replied "You figure it out."! So I demanded she pay the $10m she owed me. I have not heard from her since!