The White House chooses Paxlovid over science

Yesterday, the White house COVID czar surprisingly doubled down on Paxlovid as the silver bullet for COVID.

I was curious because most impartial observers don’t believe the totality of evidence supports Paxlovid as some type of COVID-slayer. The problem is that Paxlovid showed great benefit in unvaccinated patients in preventing progression to severe disease, but much less benefit in vaccinated/prior infected individuals.
Dr. Jha cites a study in the New England Journal of Medicine to note Paxlovid is a home run for those over 65, and despite negative results for the under 65 group in this study, cites 3 other studies that support its use in the 50-64 age group. He goes onto thread together some other studies to support his views.
It’s a really interesting thread that says a lot more about the politics of COVID than the science of COVID because it rests heavily on flawed retrospective studies of Paxlovid that show benefit, and ignores the much stronger randomized controlled trials that suggest otherwise.
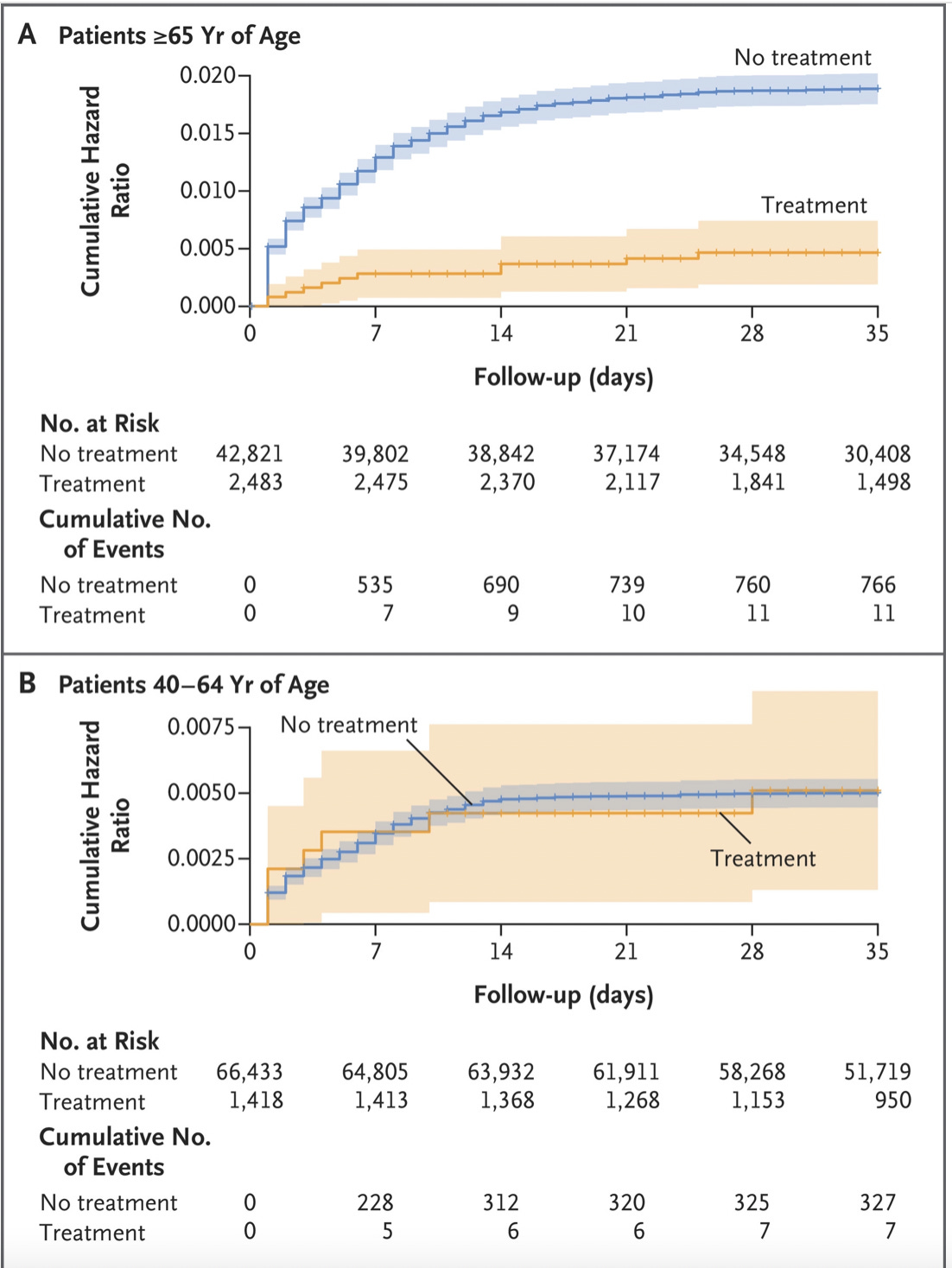
The New England Journal trial in question plumbs a large Israeli database of 1.1 million people who were infected with Sars-COV2 during the omicron surge. Approximately 109,000 were deemed high risk and eligible to receive Paxlovid. 3900 ended up receiving Paxlovid, leaving ~105,000 people who were “untreated”. Hospitalizations due to COVID were tracked in the treated and untreated group, which demonstrated significantly more hospitalizations that were judged to be due to COVID over the course of the 35 day follow up in patients > 65 years of age. No difference in hospitalizations was noted between treated and untreated groups in patients between 40-64 years of Age.
This forms the basis for COVID-czar Jha’s estimation that Paxlovid is a slam dunk for keeping patients with COVID out of the hospital. But there are a number of pitfalls in analyses like these because these are backward (retrospective) looking analyses that aren’t designed to establish causal relationships. We can never be sure in these type of retrospective studies whether there is something intrinsically different about the treated and untreated group that makes them have markedly different hospitalization rates.
For instance, as an extreme example, if it happens to be that 90% of the Paxlovid-treated group were 80 year old nursing home residents while 90% of the Paxlovid untreated group were 35 year old college kids, there’s a much higher hospitalization rate in the Paxlovid treated group that is baked in to the analysis that has nothing to do with Paxlovid.
Baseline demographic tables of the 2 groups give us some clues of the known variables that can confound the analysis, but don’t speak to confounders that are unknown, or can’t be measured. There are more diabetics in the treated group which implies the treated group is sicker, but what if the diabetics in the untreated group, while smaller in proportion had much poorer blood sugar control? One small clue in this particular dataset is the very high percentage of Israeli Arabs that are in the Paxlovid non-treated group, as it is well established that the Arab population in Israel has significantly worse health outcomes than Jews.
Another clue that the Paxlovid untreated group is intrinsically higher risk for hospitalization relates to how we would expect antibiotics and antivirals to work when it comes to reducing hospitalizations. These drugs inactivate or kill viruses/bacteria, which allows the body’s immune system to gain the upper hand and finish off the infection. The major benefit should be seen in 2-5 days after initiation of the antiviral/antibiotic. Paxlovid is given for 5 days, and there should be little impact of paxlovid beyond the 1 week mark. This is exactly what is seen in the randomized control trial of Paxlovid where we know the 2 groups being compared are identical. The large majority of the benefit with regards to hospitalizations due to COVID are seen in the first 10 days.

Compare this to the retrospective study where the two groups are not known to be the same.

In this case, benefit from Paxlovid doesn’t just end at day 10, but continues to show benefit 3-4 weeks after treatment is initiated. Its not exactly clear how hospitalizations due to COVID are adjudicated in this trial, but are we to believe that a hospitalization that occurs 21-28 days after contracting COVID is due to a COVID pneumonia? This isn’t the pattern that was seen in the randomized control trial where we know the 2 groups are identical and raises suspicions that the hospitalization difference in the treated and untreated group is less a function of Paxlovid, and more a function of intrinsic differences that aren’t being measured between the two groups.
The other issue is that the size of the positive effect in the retrospective study is not at all what was seen in the randomized control trials. While it is possible for retrospective studies to have larger effect sizes than randomized control trials, there has to be some evidence that patients who would benefit a significant amount from a therapeutic were not allowed into the randomized control trial. There is no evidence that this is happening here. So, if you had to choose between the randomized controlled trials of Paxlovid and the restropective observational studies on Paxlovid, go with the randomized control trials!
The other significant claim made that clashes with what we know about immunology, and the current available evidence on COVID is that Paxlovid’s benefit occurs irrespective of the underlying immunity status of the trial participants. In contrast, the randomized control trial Pfizer performed showed patients that had antibodies to Sars-cov2 had small to no benefit of paxlovid.


This finding was echoed in the other randomized control trial of Paxlovid performed in a vaccinated population (EPIC-SR).
"From a sample of 721 vaccinated adults with at least one risk factor for progression to severe COVID, 3/361 who received Paxlovid progressed to severe COVID compared to 7/360 patients that received placebo."
The good news here is that the randomized control trials find that severe COVID is a rare event in patients with prior immunity regardless of whether Paxlovid, ginger root or turmeric are prescribed.
Dr. Jha doesn’t mention the weak RCT evidence but does point to other retrospective studies to support the New England Journal study in his thread, giving the impression that there is strong support for a significant reduction in hospitalization and death with Paxlovid regardless of vaccination status.

Except that isn’t what the Hong Kong study says!
The supplementary table from the Hong Kong study shows that there were too few deaths in the vaccinated group and the Age < 65 group to even compare Paxlovid treated and untreated groups. So using this study to say there’s a reduction in death with Paxlovid regardless of vaccination status would be incorrect.

There are issues with the other trials Dr. Jha uses to support his stance on Paxlovid that Dr. Gellad from the University of Pittsburgh discusses as well.
In summary, the Paxlovid stance from the White House is a surprising one that doesn’t fit with the totality of data we have about Paxlovid, and seems to be grounded in the politics of COVID, rather than the science.
Most doctors would love a highly effective therapeutic for COVID, but so far, it appears that there is little additional benefit to be gained from Paxlovid in a predominantly vaccinated/recovered from COVID population.
The current administration came to power in part to rectify the wrongs of the anti-science orange man administration, and so there is a desperate need to provide a stark contrast. There needs to be “science based” activity of some kind to demonstrate how wonderful this science based administration is at crushing COVID. And so we are treated to the COVID kabuki theater of masked preschoolers, booster mandates for college kids, and pharmacists allowed to prescribe Paxlovid without a doctor involved. Already , very few people are in the hospital with COVID, but at least if we can get everyone with COVID to take Paxlovid, victory can be claimed. The science-based Paxlovid strategy is what finally crushed COVID!
But if it’s really the case that Paxlovid is minimally, or not effective at all in treating vaccinated/recovered patients, then all it takes to end COVID is a declaration from authorities that there is no longer any point in testing for COVID. (This is, by the way, exactly how the H1N1 pandemic ended.)
Unfortunately, just declaring the end without it being preceded with some public campaign (Paxlovid!) promises to be a political catastrophe for those who want credit for ending COVID and want to avoid the blame for supporting incredibly costly and damaging mitigation policies that resulted in everyone getting COVID anyway.
So it doesn’t matter that most of the country has moved on from COVID, the politics ensure a shrinking but increasingly desperate group of intellectuals will deploy a “science” smokescreen to rationalize increasingly nonsensical policies.
Don’t let them get away with it.
Anish Koka is a cardiologist. Follow him on twitter @anish_koka

Off-topic:
In case you did not come across it,
Stopping Heart Disease Progression with Dr Arthur Agatston Cardiologist Extraordinaire!
https://www.youtube.com/watch?v=R2GRuqtNTNY
The best line is the bottom line: “So it doesn’t matter that most of the country has moved on from COVID, the politics ensure a shrinking but increasingly desperate group of intellectuals will deploy a “science” smokescreen to rationalize increasingly nonsensical policies.” With midterms coming up the party in power will pull out all the steps they can and the media will support them. There is no science, only cheerleaders like Dr Jha.