Vaccine myocarditis update: Exploring the link between vaccine myocarditis and sudden cardiac death

A really interesting paper was published late November by pathologists at Heidelberg University that reviews the potential link between vaccine myocarditis and sudden death. It is interesting particularly because the ensconced narrative in academic circles and the medically related twitterati that seem to have an outsized influence on COVID related policy has been that vaccine myocarditis is “mild”.


The “mild & self-resolved” moniker refers to the experience of patients hospitalized for vaccine myocarditis. While there are case reports of severe fulminant heart failure and death, the overwhelming majority of patients appear to be able to go home a few days after presentation. The case reports of vaccine myocarditis described to date describe a typical fulminant presentation of severe myocarditis: Sudden onset of shortness of breath or chest pain, followed by rapid clinical decompensation. One of the 2 cases described in the New England Journal of Medicine was diagnosed based on autopsy findings. The pathological findings are visually fairly obvious - pink healthy cardiac tissue with islands of darkly staining immune cells associated with cell necrosis (death).

To be clear, even for the ‘mild’ cases, only in 2022 would anyone have the chutzpah to refer to mostly young adults presenting to the ER with acute severe chest pain related to vaccine caused myocardial necrosis (cell-death), two-thirds of whom go on to develop a cardiac scar on follow up, and all of whom are advised not to exercise for 6 months.. as mild.
Unfortunately, that is the line parroted from the CDC to random twitter bros who make mathematical models for a living, entirely based on the presumption that cardiac mortality from the vaccine is an exceedingly rare event. But what has been glaringly obvious for quite some time to anyone with an objective interest in the topic is that the current datasets on vaccine myocarditis only cover that group of patients who make it to the hospital.
All we have really established from the data so far is that there is a non-lethal version of vaccine myocarditis. In light of the well established concern in the cardiology community pre-pandemic that myocarditis is an important cause of sudden cardiac death, the immediate concern with all these cases of myocarditis showing up to the hospital is that there may be cases of myocarditis that result in sudden cardiac death at home, don’t make it to the hospital, and aren’t being counted.
Since the US CDC appears completely uninterested in following up concerning safety signals when it comes to the mrna vaccines (they based approval of the mrna vaccines on cardiac safety studies that were supposed to be done, but haven’t happened to my knowledge), it is left to a band of plucky German pathologists to do a meticulous study to establish the possibility vaccine myocarditis can be lethal and be missed by the current vaccine adverse event reporting systems.
The pathologists used a reporting mechanism that Germany apparently keeps for all autopsies performed in those that have died “briefly after an anti-Sars-COV2 vaccination”. Of the 54 cases of individuals dying suddenly after vaccination, 35 had autopsies performed at authors institution: Heidelberg University and forms the basis for their investigation.
Remarkably, cardiac autopsy findings consistent with myocarditis were found in five cases who were found unexpectedly dead at home within 20 days following SARS-CoV-2 vaccination.
A summary table of the decedents and the brief history available is provided below.

Person 1 was found dead 12 h after the vaccination. A witness described a rattling breath shortly before discovering circulatory failure. Person 2 complained about nausea and was found dead soon thereafter. The other persons were found dead at home without available information about terminal symptoms. According to the available information provided at the time of autopsies, none of the deceased persons had SARS-CoV-2 infection prior to vaccination and nasopharyngeal swabs were negative in all cases
Three of the deceased persons were women, two men. Median age at death was 58 years (range 46–75 years). Four persons died after the first vaccine, the remaining case after the second vaccine.
Myocarditis is thought to occur when the body’s immune system turns against healthy cardiac tissue, causing cell death. This is what has traditionally been found in classic viral myocarditis and is exactly what the German pathologists identify here as well.
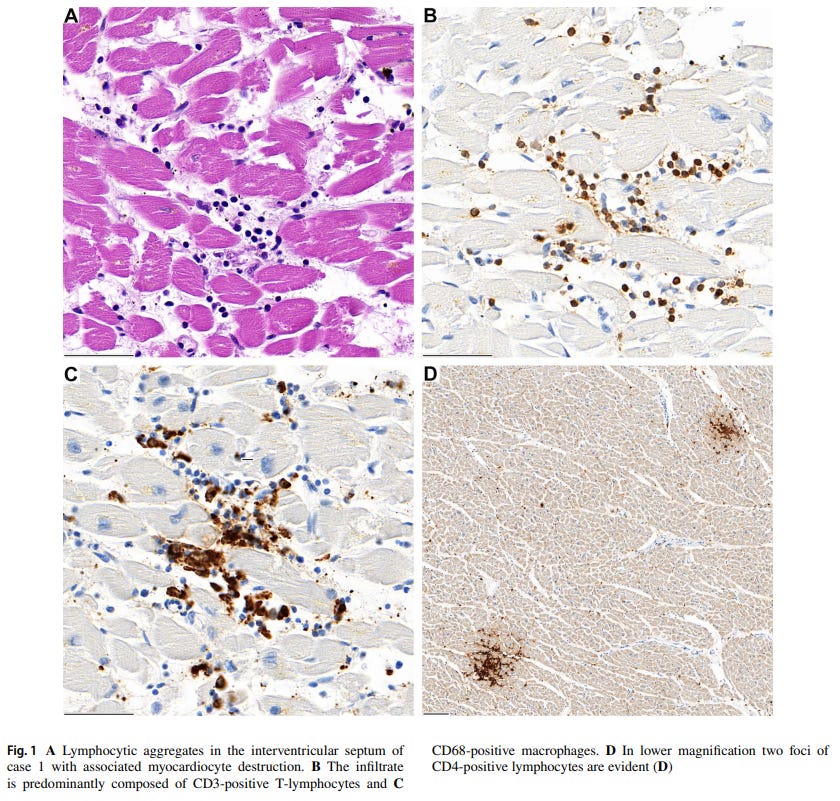
Just like the case reports depicted earlier, Panel A demonstrates healthy cardiac muscle tissue in pink, with islands of small back dots (lymphocytes) and associated cardiac destruction. Three of the 5 cases were deemed ‘likely’ myocarditis related deaths because no other plausible cause of death could be identified other than the impressive cardiac findings.
Case 5 was deemed “probable vaccine related” because the cardiac sample tested positive for low levels of a herpes virus (all autopsy samples were tested for an exhaustive panel of bacteria and viruses with PCR), while Case 3 was declared probable because the inflammatory infiltrate was found in the lining of the heart (the pericardium), rather than in the heart.
The authors are very careful to not use definitive causal terms, but it is pretty clear they strongly believe they are describing a new mechanism and novel etiology of sudden cardiac death. Support for this hypothesis comes from not one, but a number of datapoints
The close temporal relation to vaccination (all deaths occurred within one week after vaccination)
No other ‘typical’ causes of cardiac death like coronary disease, or pre-existing heart failure were noted
A negative infectious panel of other myocarditis-causing infectious agents
Presence of a peculiar receptor called CD4 was found on immune cells (T-cells) on autopsy suggestive of an immune mediated mechanism
Presence of an identical T-cell infiltrate at the deltoidal injection site in one of the cases
No comparable myocardial infiltration was found in the other 20 bodies autopsied or specimens from 3 independent historical periods that were re-analyzed
In the author’s own words:
During the last 20 years of autopsy service at Heidelberg University Hospital we did not observe comparable myocardial infammatory infiltration. This was validated by histological re-evaluation of age- and sex-matched cohorts from three independent periods, which did not reveal a single case showing a comparable cardiac pathology
Now it is not out of the realm of possibility that there just happened to be a series of ‘spontaneous’ myocarditis within days of receiving the Sars-COV2 vaccine, but the findings taken together should be highly suspicious especially in light of the reams of epidemiological data from multiple different datasets since the Spring of 2021 that clearly show the vaccines are associated with myocarditis.
It is of interest that these 5 lethal cases of presumed vaccine myocarditis are older and don’t have a male predominance, which is altogether different than the pattern observed to date in hospitalized patients (mostly young males). This could represent a survivorship bias where the health system is only seeing and recognizing the milder cases of myocarditis or may mean this is an altogether different, more lethal version of myocarditis that manifests in older individuals without the usual male predominance.
Careful researchers and experienced clinicians know better than to definitively declare anything from a 5-case autopsy report, but for anyone in charge of vaccine policy/safety to take a default position that all of these findings are completely coincidental and don’t require further investigation should be automatically disqualifying.
Further studies involving autopsy data on sudden cardiac deaths, and epidemiological data looking for a signal of increased, unexplained cardiac death (like the Florida Department of Health did here) are sorely needed to help sort this out. The earlier case reports of biopsy proven mrna vaccine myocarditis are also in an older age group and suggests clinicians and researchers should not rule out the possibility of significant myocarditis simply based on age. This is important because advancing age results in the accumulation of other comorbidities and increases the chances a severe cardiac complication could be falsely attributed to another cause. As an example, the default and reasonable assumption from the pre-pandemic era is that a 54-year-old with coronary artery disease and hypertension who died suddenly at home likely died of their pre-existing cardiac disease. In the current era, especially given the proof-of-concept German autopsy study, recent administration of a COVID vaccine should trigger an additional workup to rule out vaccine myocarditis as a cause of death.
The immediate reaction from the intellectually dark corners of social media to minimize safety concerns or dismiss reports like the one presented here as an “anti-vaxx” position is a predictable, but reflexively decerebrate reaction, because any mass vaccination campaign that relies on force rather than trust is principally wrong, and practically useless.
The German report is a meticulous, and significant addition to the body of research that has been accumulating on adverse cardiac effects from vaccines to the Sars-COV2, and should be taken seriously.
Anish Koka is a cardiologist. Follow him on twitter @anish_koka.
I have to make the obligatory post-script here that I oversaw the administration of hundreds of mrna vaccines starting in March of 2021 in my cardiology clinic. The vaccine efficacy data for the original data was from thousands of patients and I certainly felt given the devastation wreaked on many of my patients in 2020 that the vaccines were the best chance of avoiding morbidity and mortality. The process to get the vaccines from the city department of health was a somewhat arduous 3 month process, and once the vaccines were on hand, there were daily reporting requirements that I dutifully performed for the many months we were administering vaccines. To accommodate the rush of patients, employees, volunteers, and conscripted children worked multiple weekends to administer the vaccines. So I’m especially disgusted by medical colleagues who label any concerns registered about vaccine adverse events as “anti-vaxx”. Registering concern over a vaccine adverse event does not make doctors or patients “anti-vaxx”. It makes them pro-vaxx!
As a physician I have been appalled by the lack of concern of the numerous reports of possible side effects to the vaccines, and the repeated mantra of safe and effective despite what appears to be a substantial number of reactions, the uniform approach to vaccination (mandates for young adults and children despite the illness, especially since omicron, being a cold for them), the denial of natural immunity as protective, the list could go on. We can’t find what we aren’t looking for. I’m glad someone is actually looking, and thankful that you are spreading results of these studies. I no longer feel I can trust the medical establishment of our country to actually be looking out for what is best for patients.
1976 flu vaccine stopped due to 450 cases of guillian barre