

Vaccine myocarditis update from Thailand

First some background for 1st time readers. Readers who are regular followers can skip this section and go straight to the Thailand study section.
Background:
It has long ago been established that the messenger RNA vaccines cause myocarditis, the controversial question now relates to what the actual rate of myocarditis is. The CDC chart below notes a peak myocarditis rate (all boxes shaded in orange are myocarditis rates that are higher than what is expected in the population) in 16-17 year old boy of 75.9 / million (or 1/13,157 ) after dose 2 of the mrna COVID vaccine.

Unfortunately, because of the heavy reliance in the United States on passive reporting, which entails clinicians/ patients voluntarily reporting myocarditis cases, this number is likely an undercount.


Multiple datasets from around the globe from countries with much smaller budgets than our CDC have suggested higher rates than what the CDC reports. A nice comprehensive review from Hoeg, Stevenson & Krug last year demonstrates the discrepancy well.

Troublingly, the more carefully you look for myocarditis after vaccines, the more you find. Hong Kong (Chua et. al. ) has a robust surveillance system , and reported rates of myocarditis of 1/2700 in 12-17 year old boys after the 2nd dose of the Pfizer COVID vaccine. Given the Moderna vaccine has 3 times the dose of Pfizer, it is not particularly surprising that countries with access to both vaccines have noted rates of myocarditis that are 3-4x higher with Moderna than Pfizer. (French Study / Nordic Study) . This suggests that the peak rates of myocarditis with Moderna in young men could be around 1326 per million vs. the 76 per million currently reported by the CDC.
The randomized control trials were blind to this particular adverse event because there weren’t enough young men in the trial, and no one was specifically looking for this particular side effect. There are potentially a number of cases of children with chest pain that are never brought to the attention of the health care system , and are thus never captured. There is also the issues of myocardial damage that may occur without any overt, severe symptoms. The young baseball player with an ache in his left shoulder for a few days that is shrugged off. Even more concerning given the marked cardiac injury demonstrated in some vaccine myocarditis cases that presented to the hospital, it is entirely possible that there are severe cases of myocarditis that result in out of hospital death that are never labeled as myocarditis.
And it’s not just random cardiologists concerned about this. The FDA became concerned enough about myocarditis that they approved the Pfizer vaccine contingent on the performance of a number of trials specifically designed to assess the true frequency of myocarditis after administration of their vaccine. (They are supposed to report on their progress in a few weeks). One of the studies was specifically supposed to look for the “incidence of subclinical myocarditis”.

There is recent precedent for this. In response to the possibility of a smallpox bioterrorism threat from Saddam Hussein, 2 million US Service members were given a smallpox vaccine that resulted in 7x the rate of clinical myocarditis than the expected background rate. A subsequent study was then performed to assess the rate of clinical and subclinical myocarditis by routinely measuring a very sensitive blood test indicative of cardiac cell death (cardiac Troponin) after administration of the smallpox vaccine. Of the ~1000 patients in this trial, 4 developed clinical myocarditis, and 31 were found to have elevations of cardiac troponin above the 99% cutoff for a normal troponin level. The rate of cardiac injury/subclinical myocarditis was 200x the background rate of myocarditis, a rate far higher than what would have been picked up based on clinical symptoms alone.
The Thailand Study
Given the rates of myocarditis reported with the mRNA vaccines, researchers from Thailand published a preprint that enrolled 13-18 year olds in a comprehensive study that sought to assess myocardial injury by routinely checking an electrocardiogram, cardiac troponins, and an echocardiogram ( a cardiac ultrasound) at baseline and after a second dose of the Pfizer vaccine.

This is exactly the kind of study the FDA said it wanted Pfizer to do in announcing approval of the Pfizer vaccine in August of 2021. Given that the highest rates of myocarditis with the Pfizer vaccine to date have been ~ 1/3000, and the peak rate of myocarditis appears to be in the > 16 population, a study of 300 13-18 year olds from Thailand where most of the children were <15 should be fairly benign.
Unfortunately, the results are not reassuring.
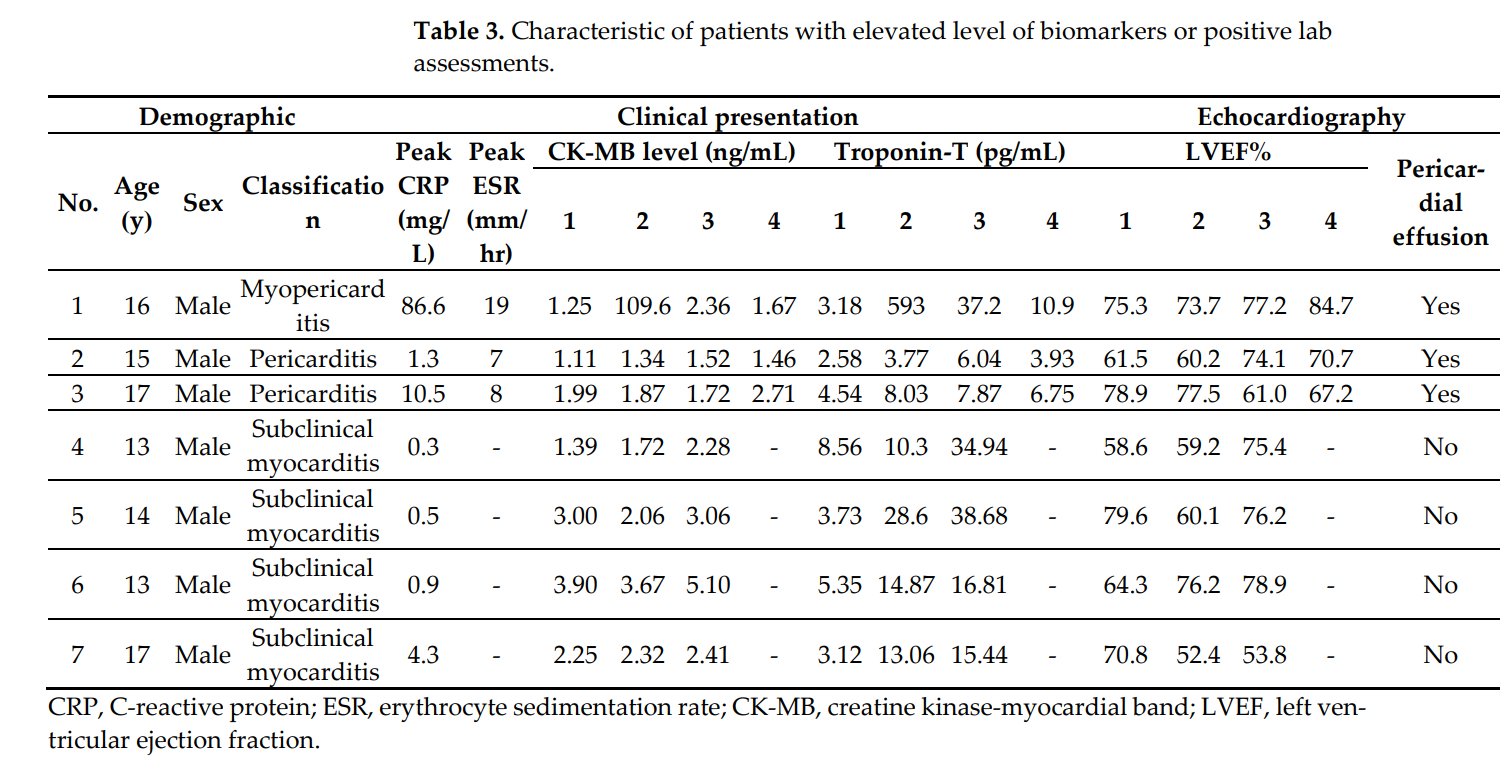
3/301 children enrolled in the study developed myocarditis or pericarditis. One 16 year old developed clinical myocarditis with a peak cardiac troponin of 593, and 2 others developed pericarditis. All three were admitted to the hospital. While it is not explicitly stated in the study, the child with myocarditis was likely monitored in the intensive care unit prior to being discharged. The one child with myocarditis appears to have had a cardiac MRI which demonstrates acute cardiac inflammation with resolution on 5 month follow up. Enhancement of the myocardium with gadolinium administration, a marker of scar formation, was not present on a 5 month follow up scan.

Four children had markers of cardiac injury that were above normal even without overt symptoms and were thus diagnosed as having subclinical myocarditis. (The troponin assay used in the study had a normal value of <14. )
It is good news that the clinical course of the vaccine series in these cases was not associated with short term severe morbidity or mortality. It is also great news that the one child with a cardiac troponin that was 40 times normal does not have evidence of significant scar formation on a cardiac MRI performed 5 months later.
But it is certainly not good news that a small 301 patient study of Thai adolescents/teenagers picks up this much cardiac injury after a second dose of the Pfizer vaccine. (Recall that the Moderna vaccine has been shown to have myocarditis rates 3-4x Pfizer). I can assure you, and the mostly ER doctor contingent on twitter that brays about “mild myocarditis”, that there are no cardiologists who want to see their child have a cardiac troponin that is 2x normal or 40x normal after administration of some therapeutic. What exactly does one to do with an adolescent with a troponin that is 2x normal that is asymptomatic? Given the theoretical risk of malignant cardiac arrhythmias I would imagine most cardiologists would follow the current guidelines for myocarditis and advise against strenuous cardiac activity for some months. Sudden cardiac death in young athletes is obviously a fearsome complication that is very real and it is likely some proportion of sudden cardiac death is from subclinical myocarditis.
We should be clear that no one currently knows the long-term significance of the clinical or subclinical myocarditis that is being diagnosed here, but there is little question in an adult population, elevations of cardiac troponin has been shown to be a poor prognostic factor. It is unclear how this relates to pediatric populations, but I don’t quite understand why anyone would want to run this experiment.
It’s important to note that the conversations I see now about elevations in troponin are completely at odds with what cardiologists have normally said in a time before the COVID vaccines rolled out. The only time cardiologists have ever minimized troponin elevations in the preCOVID era was around the performance of cardiac procedures that are associated with these elevations.
In these cases, of course, there is something wrong with a patient that needs a procedure, and the most one would say is that the benefits of the procedure outweigh the risks. It is absolutely head-spinning to see that the public conversation now is geared to dismiss cardiac injury in young healthy children as “mild”.

The issue of the risk COVID poses to the heart is a longer one beyond the scope of this article, and I’d urge readers to read my more in depth overview of the issue here, but regardless of the risk COVID poses to children, administration of a therapeutic requires an understanding of the risks of the therapy being offered. The US has done an unbelievably poor job of defining that risk to the population since myocarditis was first reported as an adverse event related to the vaccines in April of 2021. The Thai study helps fill in some of the data void so parents and their doctors can be better informed when discussing the risks and benefits of the vaccines.
Anish Koka is a cardiologist. Follow him on twitter @anish_koka
Interesting postscript:
It appears at least one country (Denmark) has decided to not routinely allow children under 18 to get the vaccine, unless approved by a physician.


I have to make the obligatory post-script here that I oversaw the administration of hundreds of mrna vaccines starting in March of 2021 in my cardiology clinic. The vaccine efficacy data for the original data was from thousands of patients and I certainly felt given the devastation wreaked on many of my patients in 2020 that the vaccines were the best chance of avoiding morbidity and mortality. The process to get the vaccines from the city department of health was a somewhat arduous 3 month process, and once the vaccines were on hand, there were daily reporting requirements that I dutifully performed for the many months we were administering vaccines. To accommodate the rush of patients, employees, volunteers, and conscripted children worked multiple weekends to administer the vaccines. So I’m especially disgusted by medical colleagues who label any concerns registered about vaccine adverse events as “anti-vaxx”. Registering concern over a vaccine adverse event does not make doctors or patients “anti-vaxx”.
Why are doctors still trying to save this vaccine program, especially when the boosted appear to get recurrent infections? Is it willful blindness, like Dr. McCullough suggests? Since so many doctors (not me, thank God) got the shot, maybe they cannot admit that they probably made a mistake? Most kids are already immune. Are there any studies worldwide that study myocarditis risk in kids who already had immunity vs. those who did not? That would be interesting to know.
Well written.
The long terms of these myocarditis injuries are "unknown" but if we read the literature "The mortality rate is up to 20% at 1 year and 50% at 5 years. Despite optimal medical management, overall mortality has not changed in the last 30 years." https://www.ncbi.nlm.nih.gov/books/NBK459259/