

FAQs about the Thailand Vaccine myocarditis post
Overdiagnosis, control arms, subclinical myocarditis and more..

There were some good questions generated by my post on the vaccine myocarditis study from Thailand. I thought I’d try to flesh them out for people interested.
The study had no control arm. How can you say anything about the vaccine causing anything without a control arm?
We already know based on more than a year’s worth of data and multiple datasets that the messenger RNA vaccines cause myocarditis. This is about as settled as you can get in science today. At this point there is no health agency in the world that does not causally link the messenger RNA COVID vaccine with myocarditis, so we do not need a control arm to establish whether or not myocarditis happens after the vaccines. What we do need is to establish the rate of myocarditis after delivery of the mrna vaccines. Relying on a voluntary reporting system will undercount cases of myocarditis, so an important study to do is a prospective study of myocardial injury in a cohort of individuals who are given the vaccine. This is the very study that the FDA has asked Pfizer to do as well! Also, important to note that when the smallpox vaccine rollout was associated with high rates of myocarditis, the same study design was used to assess myocardial injury after the smallpox vaccine.
Short answer: A control arm isn’t needed when trying to establish the rate of an established adverse event.
Is troponin elevation normal after the administration of most vaccines?
Troponin elevations occur in the presence of cardiac cell death. Some vaccines are associated with myocarditis and others are not. There is no causal link for myocarditis with the MMR shot or the Flu shot (as examples). There is a causal link with the smallpox vaccine and the COVID vaccines. Interestingly, the prospective smallpox study did have a control arm where some recipients received the flu vaccine. No patients who received the flu vaccine had any cases of clinical or subclinical myocarditis. The only reason prospective studies of subclinical myocarditis are being asked for by the FDA in this case is because there is an established link between clinical myocarditis and the current mRNA vaccines. This is NOT a random search of troponin elevations after vaccine administration.
Short answer: No, troponin elevations are not normal after vaccine administration.
Aren’t some troponin elevations clinically insignificant?
A troponin assay is a quantitative measure of cardiac cell death. The higher the troponin, the more cardiac cells that are considered to be damaged (usually irreversibly) and the worse prognosis is. Almost all troponin assays in use today report abnormal values that are >99th percentile of normal. This means that every assay that is approved for use has a normal reference range based (of course) on a normal population. An abnormal troponin means having a value that is above the 99th percentile of a normal population.
In the Thai study a troponin (Tn) assay > 14 was abnormal, which means a Tn > 14 is above the 99th percentile of normal for that particular assay. The one case of symptomatic myocarditis found out of a sample of 300 13-18 years olds had a peak troponin of 500. This is >40 times the normal reference range. While some lay people may be understandably perplexed or confused about this, no practicing cardiologist with a functioning brain thinks this is clinically insignificant.
There were 4 cases of subclinical myocarditis noted in the study based on troponin elevations. In my post, I noted two of these cases had troponin elevations that were two times the normal reference range. I also note in my post that while it is unclear what this means long term, no cardiologist thinks their child developing a troponin that is 2 times the normal reference range because of a vaccine they may have been forced to take to attend college is desirable.
At the end of the day, a dataset of 301 young children 13-18 years old, with 202 boys, there was 1 clinical case of myocarditis, 2 cases of pericarditis, and at least 2 case of troponin elevations that were multiples of the normal troponin reference range.
Short answer: The troponin elevations I highlighted in the post are significant, and that this happened in a dataset of only 300 13-18 year old’s is concerning
What would your response be to troponin elevations checked after a COVID infection?
We already know the answer to this question. First, COVID is not known to cause acute myocarditis in children. The myocarditis reported in children related to COVID relates to a process called MIS-C which is thought to be an autoimmune process that occurs well after resolution of the acute COVID infection. In cases of MIS-C, troponin elevations are found to be far less than what’s seen in vaccine related myocarditis. This case series from Oster, et. al., found zero cases of covid myocarditis (classic myocarditis were historical cases of classic myocarditis), MIS-C myocarditis that basically had close to zero troponin elevation, and vaccine myocarditis cases with far greater troponin elevations than MIS-C myocarditis cases. (It also needs to be said that MIS-C did not occur after the large, massive COVID wave in children in the winter of 2021, so the risk of MIS-c to children may be declining significantly over time)
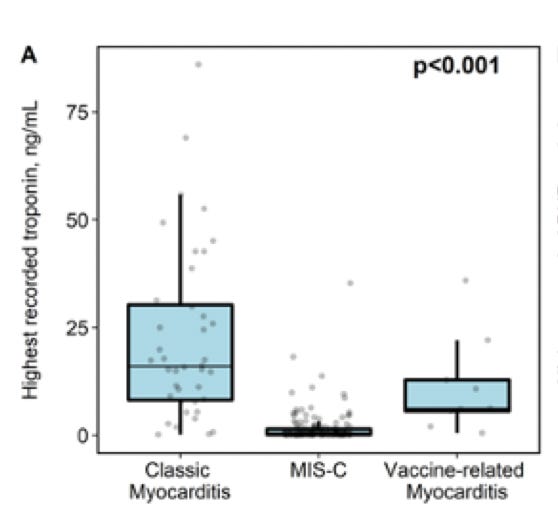
Short answer: This experiment has been run. In children, cardiac injury after acute COVID infections luckily doesn’t appear to happen. MIS-C myocarditis which is thought to be a post COVID phenomenon has nowhere close to the cardiac injury seen compared to vaccine myocarditis
Is the Thailand study an example of ‘overdiagnosis’?
Overdiagnosis is a major problem in medicine today that is a function of too-sensitive tests being developed that may actually be redefining normal to abnormal. A good example of overdiagnosis is the performance of cardiac MRI studies in a series of patients that had recovered from COVID. These studies essentially found bright spots occurring in a significant percentage of these patients which lead the academic researchers to declare cardiac injury after COVID was rampant.
But none of this was grounded in reality. There was no tsunami of patients with acute covid going to the ER with chest pain and elevated troponins and there was no tsunami of patients coming to cardiologists in the midst of massive outbreaks in US cities with complaints of clinical myocarditis.
The MRI COVID myocarditis saga was a nice example of overdiagnosis, or fabrication of an illness. It would be a mistake to conflate a young child with chest pain and a troponin of 500 with bright spots found on MRIs performed on a random series of people recovered from COVID.
Short answer: Significant elevations in troponins that are reflective of cardiac cell death caused by a vaccine isn’t overdiagnosis.
What do you make of the ECG abnormalities reported by the authors?
Not much. Why I didn’t mention the ECGs in my post. The much more significant finding are the clinical cases of myocarditis and the significant troponin elevations.
What can we say about the rates of myocarditis based on this study?
Putting this study in the context of the global dataset to date, it suggests that rates of myocarditis in young men is many times higher that what has been reported by the US CDC. This is also the first study to date to demonstrate significant asymptomatic elevations of a blood test that is sensitive for cardiac cell death. This is one study, and the results do need to be replicated.
What are the long-term implications of subclinical myocarditis as defined in this study?
It is not known what the long-term significance of troponin elevations at a subclinical level are, but it is an important finding to discuss with patients, and parents so that the risks and benefits of the vaccine can be contextualized to the individual patient. Troponin elevations occur because of cardiac cell death. The higher the troponin levels, the more cardiac cells that die, and the worse the long-term prognosis. As I note in my post, it is possible this is associated with a benign prognosis, but it strikes me as a crazy experiment to run on millions of children if there are other options. There is also no guarantee, of course that your child will have a 1.2x, 2x elevation in cardiac troponin or a 40x elevation in cardiac troponin (the range in the Thailand study I highlighted). At the very least, this is all a conversation worth having with parents.
Short answer: We don’t know. (But it doesn’t seem like a really smart experiment to run)
Is sub clinical myocarditis made up?
Yes and No. Sudden cardiac arrest, especially in young healthy athletes, is a devastating complication and it does seem likely that some unknown percentage of these tragic cases have sub clinical myocarditis as a cause. The belief is that small amounts of scar or irritation that develop in the heart may trigger lethal arrhythmias during strenuous exercise. Singapore recommended vaccinated individuals avoid strenuous exercise for a week after vaccination because of reports of myocarditis and a teenager that suffered cardiac arrest while playing sports. We can quibble about what troponin level constitutes myocarditis vs. cardiac injury after administration of a vaccine, but there are very few cardiologists that would dismiss marked elevations of a marker of cardiac cell death as “insignificant”
Short answer: Yes and No. But the important point remains that significant cardiac injury after the administration of any therapeutic is not an insignificant finding.
What about the long-term implications of abnormal cardiac MRI findings that have been reported after getting COVID?
The cardiac MRI findings, like all findings in cardiac imaging, exist across a continuum. The findings seen on cardiac MRI to date after can best be classified as mild. If it was the case that cardiac MRIs on patients who had COVID actually showed 20% of the heart muscle being replaced by scar, I would be telling a very different story. A recent paper that was amplified by cardiology influencer and former Theranos booster Eric Topol is a great example of the subtle MRI findings that can be converted to COVIDpanic gold on social media but is actually just hyperbolic shit. I’ll repeat myself just because it’s important to drive home: MRI T1 abnormalities and scattered bright spots in a group of people that think they had COVID is in no way analogous to troponin elevations that range from 2x to 40x normal in young healthy children.
Even if the findings on MRI after COVID were in any way comparable to the troponin elevations that can result from vaccine myocarditis (they are not), there is still the ethical quandary of a vaccine being mandated to participate in society causing injury vs. the injury that comes from getting COVID as one participates in normal life activities.
Short answer: It is very unlikely that the abnormal findings seen so far on cardiac MRIs after COVID are clinically significant.

Anish Koka is a cardiologist. Follow him @anish_koka.
Also important context about the conversation in some locales about children and vaccines :

Thank you for this summary. Can you explain (or hypothesize) why the mRNA vaccine would cause cardiac cell damage (or elevated troponin levels) in some children but not others? Indeed, 295 of the 300 children didn't have elevated levels. But why were those 5 children so unlucky?
Please know that I'm not in any way trying to minimize a rate of 5 out of of 300 children--it's an insane risk to take for no apparent benefit, in my opinion--but it's something I've been curious about regarding vaccine injuries generally.
I'd be grateful for any insight you have.
Here is my response:
https://sanjayverma-66740.medium.com/it-doesnt-matter-what-i-believe-it-only-matters-what-i-can-prove-87130a10e39e